
Lymphogranuloma Venereum Proctocolitis (LVG) is a disease caused by a bacteria called Chlamydia trachomatis.
The bacterium comes in three variations, L1, L2, and L3, and is transmitted sexually.
In Africa, the condition is prevalent among men who have sex with other men and women receptive to anal sex.
Prevalence of the disease in Africa
World Health Organization (WHO) estimates show that 10 million people infected with LVG are from the sub-Saharan part of Africa.
The majority of these infections are from Nigeria and South Africa.
In Nigeria, 5.2% of the men who had sex with other men and had an STI infection also tested positive for LVG, although none reported any symptoms.
Furthermore, 71% of Nigerian men who practice same-sex and had tested positive for LVG, also tested positive for HIV.
Homosexual immigrant workers from the southern part of Africa, Lesotho, Swaziland, and Botswana suffer the most from LVG infections.
The infections are also common in the rural regions of Mpumalanga, Eastern Cape, and Kwa-Zulu-Natal.
Other African countries with significant numbers of infections include Zambia and Malawi. Zambia has a 3% occurrence of LVG among women visiting health centers to receive treatment.
Malawi has a 6% prevalence of the disease.
Symptoms
African women are mostly asymptomatic, and the disease becomes apparent only when the effects check-in.
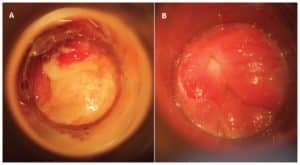
A painful inflammation appears in the rectum among most men within thirty days after the infection.
The swelling is characteristic of bleeding, pus, ulcers, and constipation.
The symptoms also include a fever, a rash on your neck, groin, or armpit.
Diagnosis
The first step in diagnosis is mostly clinical suspicion after ruling out all the other genital ulcer diseases. After that, a serology test of the rectal, lymph nodes, or genital specimens follows.
Effects of the Disease
LVG infections among women may cause infections of the cervix, the endometrium, the fallopian tubes, and the pelvis.
Untreated infections also cause low birth weight, premature rupturing of the membranes, conjunctivitis among newborns and neonatal sepsis.
LVG is also linked with 85% of infertility among women who attend infertility clinics.
Mode of infection
LVG infections in African spiked after the number of men having sex with other men increased, as well as the number of women receptive to anal sex.
That is because all the three variations of the infection, Chlamydia trachomatis L1, L2, and L3 are transmitted upon contact with ulcerations, or skin with tears, or if ingested orally.
Treatment
The management of the disease in Africa is syndromic – meaning, the treatment is not specific to the disease, but rather alongside other conditions with near similar symptoms.
And therefore, the infections and its effects are still a threat in most of Africa.
The treatment of the disease in Africa includes the use of antibacterials for a period of twenty-one days.
Conclusion – LVG in Africa
Although LVG is still endemic in Africa, most infections are among homosexuals, heterosexual women receptive to anal sex, and HIV positive individuals.
It is treatable. However, the use of condoms and practicing safe sex are the best methods to minimize its spread.